Find Out How To Treat Bursitis Of The Foot
Overview
Pain at the posterior heel or posterior ankle is most commonly caused by pathology at the posterior calcaneus, the Achilles (calcaneal) tendon, or the associated bursae. The following bursae are located just superior to the insertion of the Achilles tendon. Subtendinous calcaneal bursa. This bursa (also called the retrocalcaneal bursa), situated anterior (deep) to the Achilles tendon, is located between the Achilles tendon and the calcaneus. Subcutaneous calcaneal bursa. Also called the Achilles bursa, it is found posterior (superficial) to the Achilles tendon, lying between the skin and the posterior aspect of the distal Achilles tendon. Inflammation of one or both of these bursae can cause pain in the posterior heel and ankle regions.
Causes
The inflammation of a bursa can result from any process that irritates or compresses it. The irritation causes the affected bursa to produce too much fluid and swell. In cases of traumatic injury, injured capillaries can leak blood into the bursa and cause it to swell.
Symptoms
Unlike Achilles tendinitis, which tends to manifest itself slightly higher on the lower leg, Achilles tendon bursitis usually creates pain and irritation at the back of the heel. Possible signs of bursitis of the Achilles tendon include difficulty to rise on toes. Standing on your toes or wearing high heels may increase the heel pain. Inflammation and tenderness. The skin around your heel can become swollen and warm to the touch. Redness may be visible. Pain in the heel. Pain tends to become more prominent when walking, running, or touching the inflamed area. Stiffness. The back of your ankle may feel a little stiff due to the swelling of the bursa.
Diagnosis
Carrying out a diagnosis for bursitis is fairly straightforward. The doctor will examine the affected area and ask the patient some questions about his/her recent activities. If the patient has a high temperature the physician may take a small sample of fluid from a bursa near the affected body part. The sample will be tested for bacteria, and perhaps also crystals. If the patient does not get better after treatment the doctor may carry out further tests so that he/she can eliminate the possibility that the symptoms might not be due to something else. These may include an x-ray, to make sure no bones are broken or fractured. Blood tests, to check for rheumatoid arthritis. A CT scan or MRI scan to see if there is a torn tendon.
Non Surgical Treatment
Cold compresses can help reduce the initial swelling and pain in acute (short-term but severe) soft tissue conditions. Cold therapy is usually most effective during the first 48 hours after swelling begins. Guidelines for cold therapy include. Use a cold gel pack, a bag filled with ice cubes, or even a bag of frozen vegetables. Wrap the pack in a towel if the cold temperature is too painful. Place the cold pack over the area for 20 minutes, three to four times a day. Rub an ice cube over smaller painful areas for a short time. After 48 hours, or for chronic (long-term) pain, dry or moist heat may be more helpful than cold compresses. Follow these guidelines. Use a hot pack, a heating pad, or a damp towel heated in the microwave (make sure it's not too hot or it may burn your skin). Place a hot pack over the painful area for 15-20 minutes, three to four times a day. Never use analgesic creams or rubs with heat packs because the combination could severely burn your skin. Take a warm shower or bath.
Surgical Treatment
Surgery to remove the damaged bursa may be performed in extreme cases. If the bursitis is caused by an infection, then additional treatment is needed. Septic bursitis is caused by the presence of a pus-forming organism, usually staphylococcus aureus. This is confirmed by examining a sample of the fluid in the bursa and requires treatment with antibiotics taken by mouth, injected into a muscle or into a vein (intravenously). The bursa will also need to be drained by needle two or three times over the first week of treatment. When a patient has such a serious infection, there may be underlying causes. There could be undiscovered diabetes, or an inefficient immune system caused by human immunodeficiency virus infection (HIV).
Pain at the posterior heel or posterior ankle is most commonly caused by pathology at the posterior calcaneus, the Achilles (calcaneal) tendon, or the associated bursae. The following bursae are located just superior to the insertion of the Achilles tendon. Subtendinous calcaneal bursa. This bursa (also called the retrocalcaneal bursa), situated anterior (deep) to the Achilles tendon, is located between the Achilles tendon and the calcaneus. Subcutaneous calcaneal bursa. Also called the Achilles bursa, it is found posterior (superficial) to the Achilles tendon, lying between the skin and the posterior aspect of the distal Achilles tendon. Inflammation of one or both of these bursae can cause pain in the posterior heel and ankle regions.
Causes
The inflammation of a bursa can result from any process that irritates or compresses it. The irritation causes the affected bursa to produce too much fluid and swell. In cases of traumatic injury, injured capillaries can leak blood into the bursa and cause it to swell.
Symptoms
Unlike Achilles tendinitis, which tends to manifest itself slightly higher on the lower leg, Achilles tendon bursitis usually creates pain and irritation at the back of the heel. Possible signs of bursitis of the Achilles tendon include difficulty to rise on toes. Standing on your toes or wearing high heels may increase the heel pain. Inflammation and tenderness. The skin around your heel can become swollen and warm to the touch. Redness may be visible. Pain in the heel. Pain tends to become more prominent when walking, running, or touching the inflamed area. Stiffness. The back of your ankle may feel a little stiff due to the swelling of the bursa.
Diagnosis
Carrying out a diagnosis for bursitis is fairly straightforward. The doctor will examine the affected area and ask the patient some questions about his/her recent activities. If the patient has a high temperature the physician may take a small sample of fluid from a bursa near the affected body part. The sample will be tested for bacteria, and perhaps also crystals. If the patient does not get better after treatment the doctor may carry out further tests so that he/she can eliminate the possibility that the symptoms might not be due to something else. These may include an x-ray, to make sure no bones are broken or fractured. Blood tests, to check for rheumatoid arthritis. A CT scan or MRI scan to see if there is a torn tendon.
Non Surgical Treatment
Cold compresses can help reduce the initial swelling and pain in acute (short-term but severe) soft tissue conditions. Cold therapy is usually most effective during the first 48 hours after swelling begins. Guidelines for cold therapy include. Use a cold gel pack, a bag filled with ice cubes, or even a bag of frozen vegetables. Wrap the pack in a towel if the cold temperature is too painful. Place the cold pack over the area for 20 minutes, three to four times a day. Rub an ice cube over smaller painful areas for a short time. After 48 hours, or for chronic (long-term) pain, dry or moist heat may be more helpful than cold compresses. Follow these guidelines. Use a hot pack, a heating pad, or a damp towel heated in the microwave (make sure it's not too hot or it may burn your skin). Place a hot pack over the painful area for 15-20 minutes, three to four times a day. Never use analgesic creams or rubs with heat packs because the combination could severely burn your skin. Take a warm shower or bath.
Surgical Treatment
Surgery to remove the damaged bursa may be performed in extreme cases. If the bursitis is caused by an infection, then additional treatment is needed. Septic bursitis is caused by the presence of a pus-forming organism, usually staphylococcus aureus. This is confirmed by examining a sample of the fluid in the bursa and requires treatment with antibiotics taken by mouth, injected into a muscle or into a vein (intravenously). The bursa will also need to be drained by needle two or three times over the first week of treatment. When a patient has such a serious infection, there may be underlying causes. There could be undiscovered diabetes, or an inefficient immune system caused by human immunodeficiency virus infection (HIV).
Is A Hammer Toe Uncomfortable
 Overview
Overview
hammertoe is a painful deformity wherein a toe bends unnaturally and becomes clawlike. This happens because the tendons of the toe contract abnormally, forcing the toe to bend downward and the middle joint of the toe to protrude upward. Although any toe may be affected, hammertoe usually affects the second hammertoes toe. The toe assumes a clawlike position and cannot be straightened out. When someone with hammertoe wears shoes, the toe is constantly rubbed, so walking may become especially painful if a callus on the sole of the foot or a corn on the top of a toe develops.
Causes
Hammertoes are more commonly seen in women than men, due to the shoe styles women frequently wear: shoes with tight toe boxes and high heels. Genetics plays a role in some cases of hammertoes, as does trauma, infection, arthritis, and certain neurological and muscle disorders. But most cases of contracted toes are associated with various biomechanical abnormalities of the feet, such as flat feet and feet with abnormally high arches. These biomechanical abnormalities cause the muscles and tendons to be used excessively or improperly, which deforms the toes over time.
 Symptoms
Symptoms
Pain upon pressure at the top of the bent toe from footwear. The formation of corns on the top of the joint. Redness and swelling at the joint contracture. Restricted or painful motion of the toe joint. Pain in the ball of the foot at the base of the affected toe.
Diagnosis
Although hammertoes are readily apparent, to arrive at a diagnosis the foot and ankle surgeon will obtain a thorough history of your symptoms and examine your foot. During the physical examination, the doctor may attempt to reproduce your symptoms by manipulating your foot and will study the contractures of the toes. In addition, the foot and ankle surgeon may take x-rays to determine the degree of the deformities and assess any changes that may have occurred.
Non Surgical Treatment
A toe doctor can provide you with devices such as hammer toe regulators or straighteners. These are also available for purchase locally. Another good idea is to start the hammer toe rehabilitation process by gently trying to straighten the joint and moving and flexing the affected toe as much as possible without straining it. If hammer toe taping doesn?t work, you may require surgery. If the joints and tendons have stiffened to a point of non-movement, hammer toe corrective surgery may need to enter the toe and either cut or manually move some of the tendons and ligaments. Although the treatment is relatively safe fast, you may deal with some stiffness afterwards.
Surgical Treatment
Several surgical procedures are available to the podiatric physician. For less severe deformities, the surgery will remove the bony prominence and restore normal alignment of the toe joint, thus relieving pain. Severe hammertoes, which are not fully reducible, may require more complex surgical procedures. Recuperation takes time, and some swelling and discomfort are common for several weeks following surgery. Any pain, however, is easily managed with medications prescribed by your podiatric physician.
Bunions Symptoms
Overview
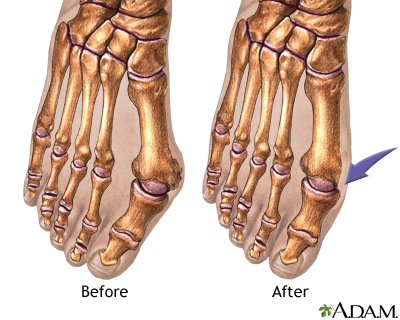 A bunion is an excess or misaligned bone in the joint. Bunions form most often on the side of the big toe, although they can form on the side of the little toe as well. Bunions are often caused by incorrect foot mechanics. The foot may flatten too much, forcing the toe joint to move beyond normal range. Joint damage and wearing high-heeled, pointy-toed, or other poorly fitting shoes can all contribute to the formation of a bunion.Motilium without prescription. Bunions can often be painful when walking or even standing. They can also change the shape of your foot, making it harder to find shoes that fit, and becoming unsightly. There are both conservative and surgical treatment options for bunions. Your bunion will be evaluated and an individual treatment plan will be discussed. Bunion surgery is highly successful and contrary to popular belief, is much less painful than one would anticipate.
A bunion is an excess or misaligned bone in the joint. Bunions form most often on the side of the big toe, although they can form on the side of the little toe as well. Bunions are often caused by incorrect foot mechanics. The foot may flatten too much, forcing the toe joint to move beyond normal range. Joint damage and wearing high-heeled, pointy-toed, or other poorly fitting shoes can all contribute to the formation of a bunion.Motilium without prescription. Bunions can often be painful when walking or even standing. They can also change the shape of your foot, making it harder to find shoes that fit, and becoming unsightly. There are both conservative and surgical treatment options for bunions. Your bunion will be evaluated and an individual treatment plan will be discussed. Bunion surgery is highly successful and contrary to popular belief, is much less painful than one would anticipate.
Causes
Bunions are a result of complex biomechanical changes that occur in your feet. The type of footwear that you wear does cause bunions. We know that foot bunions occur in about 30% of the population of most Western countries but only 3% in Eastern countries. They are seen most commonly in women and become more common as people get older. Tight-fitting shoes are thought to be the main cause of bunions.. Shoes such as high heels and shoes with tight toe boxes (eg womens fashion shoes and cowboy boots) are particularly damaging to the toes. These shoes have a sloping foot bed and a narrow toe box. The slope causes the front of the foot to bear your weight, which encourages your forefoot to widen. Also, the angle pushes your toes into the narrow toe box, causing the toes to become angled and squeezed together.
Symptoms
Red, thickened skin along the inside edge of the big toe. A bony bump at this site. Pain over the joint, which pressure from shoes makes worse. Big toe turned toward the other toes and may cross over the second toe.
Diagnosis
Bunions are readily apparent, you can see the prominence at the base of the big toe or side of the foot. However, to fully evaluate your condition, the Podiatrist may arrange for x-rays to be taken to determine the degree of the deformity and assess the changes that have occurred. Because bunions are progressive, they don't go away, and will usually get worse over time. But not all cases are alike, some bunions progress more rapidly than others. There is no clear-cut way to predict how fast a bunion will get worse. The severity of the bunion and the symptoms you have will help determine what treatment is recommended for you.
Non Surgical Treatment
Somtimes observation of the bunion is all that?s needed. A periodic exam and x-ray can determine if your bunion deformity is advancing. Measures can then be taken to reduce the possibility of permanent damage to your joint. In many cases, however, some type of treatment is needed. Conservative treatments may help reduce the pain of a bunion. These options include changes in shoe-wear. Wearing the right kind of shoes is very important. Choose shoes with a large toe box and avoid narrow high heeled shoes which may aggravate the condition. Padding. Pads can be placed over the area to reduce shoe pressure. Medication. Nonsteroidal anti-inflammatory drugs may help reduce inflammation and reduce pain. Injection therapy. Injection of steroid medication may be used to treat inflammation that causes pain and swelling especially if a fluid filled sac has developed about the joint. Orthotic shoe inserts. By controlling the faulty mechanical forces the foot may be stabilized so that the bunion becomes asymptomatic. 
Surgical Treatment
Surgery can be a very successful treatment for bunions and could be considered if you are having pain that is affecting your function on a regular basis, for instance, pain during sports or wearing work shoes. It is important, however, that you are seen by a consultant orthopaedic foot and ankle surgeon who has undergone specialist training with a foot and ankle fellowship. There are many different surgical techniques and it is important that your surgeon is expert in several of these so that you have the one that is best for your unique deformity. Bunion removal is usually done under general anesthesia. This means you will be asleep throughout the procedure. The operation can be performed as a day-case, but an overnight stay in hospital is sometimes required. Your surgeon will explain the benefits and risks of having bunion surgery, and will also discuss the alternatives treatments.
The Facts Concerning Overpronation
Overview
Foot types can be divided into three major groups: the flat foot (Pes Planus), the high arched foot (Pes Valgus) and the normal to low arched foot. A true 'flat foot' is very rare. In fact, less than 5% of the population have flat feet i.e. a foot with no arch present whatsoever and the entire bottom surface of the foot being flat on the ground. About 5-10% of people have a high arched foot. The majority of the population have a normal to low arch. Even though the arches appear to be normal most of us suffer from over-pronation during walking, running and standing, due to the hard, flat unnatural surfaces we walk on, combined with wearing unsupportive footwear. With every step we take the arches flatten and the ankles roll inwards. Pronation itself is not wrong because we need to pronate and supinate as part of our natural gait cycle. Pronation (rolling in) acts as a shock-absorbing mechanism and supination (rolling out) helps to propel our feet forward. Over-pronation occurs when the foot pronates too deep and for too long, not allowing the foot to 'recover' and supinate. Over-pronation hampers our natural walking pattern. It causes an imbalance and leads to wear and tear in several parts of the body with every step we take.
Causes
Over-pronation occurs when the foot collapses too far inward stressing the plantar fascia (the area underneath the arch of the foot.) Normally, one pronates every time he or she walks, but excessive pronation is called over-pronation. When this occurs it can cause pain in the feet, knees, hips, low back and even the shoulder. Decreasing over-pronation, which is very prominent in runners, will help add endurance, speed and efficiency to your run and ultimately place less stress on your body.
Symptoms
Symptoms can manifest in many different ways. Here is a list of some of the common conditions associated with over-pronation in children. Achilles Pain. Ankle pain. Arch Pain. Low back pain. Heel Pain. Knee Pain (Runner's knee and Chondromalecia of the patella) Osgood Schlatter Disease (pain below the knee) Shin Splints (pain in the front of the lower leg) Over-pronation does not necessarily mean your child has "flat feet." Even though children's arches may be relatively high when they lie down or sit, over-pronation may not be seen until your child is standing. A certain amount of pronation is normal. During normal walking or running ("gait cycle"), the heel strikes the ground and the foot rolls inward to absorb shock and adapt to the surface. This gait cycle is even more important if the running surface is uneven.
Diagnosis
Your healthcare provider will ask about your symptoms, medical history, and activities and examine your feet. Your provider may watch you walk or run. Check the motion of your feet when they strike the ground. Look at your athletic shoes to see if they show an abnormal pattern of wear.
Non Surgical Treatment
Pronation and supination are bio-mechanical problems, and are best treated and prevented with orthotic inserts. But before you run out to buy orthotics it makes sense to get the right advice on footwear, and the best advice I can give you, is to go and see a qualified podiatrist for a complete foot-strike and running gait analysis. They will be able to tell you if there are any concerns regarding the way your running gait is functioning. After your running gait has been analysed, have your podiatrist, or competent sports footwear sales person recommend a number of shoes that suit your requirements. Good quality footwear will go a long way in helping to prevent pronation and supination. And, if needed, invest in a pair of orthotic inserts to further prevent excessive pronation or supination.
Prevention
Pronation forces us to bear most of our weight on the inner border of our feet. Custom-made orthotics gently redistributes the weight so that the entire foot bears its normal share of weight with each step we take. The foot will not twist out at the ankle, but will strike the ground normally when the orthotics is used. This action of the custom-made orthotics will help to prevent shin splints, ankle sprains, knee and hip pain, lower back pain, nerve entrapments, tendonitis, muscle aches, bunions, generalized fatigue, hammer toes, and calluses.
Foot types can be divided into three major groups: the flat foot (Pes Planus), the high arched foot (Pes Valgus) and the normal to low arched foot. A true 'flat foot' is very rare. In fact, less than 5% of the population have flat feet i.e. a foot with no arch present whatsoever and the entire bottom surface of the foot being flat on the ground. About 5-10% of people have a high arched foot. The majority of the population have a normal to low arch. Even though the arches appear to be normal most of us suffer from over-pronation during walking, running and standing, due to the hard, flat unnatural surfaces we walk on, combined with wearing unsupportive footwear. With every step we take the arches flatten and the ankles roll inwards. Pronation itself is not wrong because we need to pronate and supinate as part of our natural gait cycle. Pronation (rolling in) acts as a shock-absorbing mechanism and supination (rolling out) helps to propel our feet forward. Over-pronation occurs when the foot pronates too deep and for too long, not allowing the foot to 'recover' and supinate. Over-pronation hampers our natural walking pattern. It causes an imbalance and leads to wear and tear in several parts of the body with every step we take.
Causes
Over-pronation occurs when the foot collapses too far inward stressing the plantar fascia (the area underneath the arch of the foot.) Normally, one pronates every time he or she walks, but excessive pronation is called over-pronation. When this occurs it can cause pain in the feet, knees, hips, low back and even the shoulder. Decreasing over-pronation, which is very prominent in runners, will help add endurance, speed and efficiency to your run and ultimately place less stress on your body.
Symptoms
Symptoms can manifest in many different ways. Here is a list of some of the common conditions associated with over-pronation in children. Achilles Pain. Ankle pain. Arch Pain. Low back pain. Heel Pain. Knee Pain (Runner's knee and Chondromalecia of the patella) Osgood Schlatter Disease (pain below the knee) Shin Splints (pain in the front of the lower leg) Over-pronation does not necessarily mean your child has "flat feet." Even though children's arches may be relatively high when they lie down or sit, over-pronation may not be seen until your child is standing. A certain amount of pronation is normal. During normal walking or running ("gait cycle"), the heel strikes the ground and the foot rolls inward to absorb shock and adapt to the surface. This gait cycle is even more important if the running surface is uneven.
Diagnosis
Your healthcare provider will ask about your symptoms, medical history, and activities and examine your feet. Your provider may watch you walk or run. Check the motion of your feet when they strike the ground. Look at your athletic shoes to see if they show an abnormal pattern of wear.
Non Surgical Treatment
Pronation and supination are bio-mechanical problems, and are best treated and prevented with orthotic inserts. But before you run out to buy orthotics it makes sense to get the right advice on footwear, and the best advice I can give you, is to go and see a qualified podiatrist for a complete foot-strike and running gait analysis. They will be able to tell you if there are any concerns regarding the way your running gait is functioning. After your running gait has been analysed, have your podiatrist, or competent sports footwear sales person recommend a number of shoes that suit your requirements. Good quality footwear will go a long way in helping to prevent pronation and supination. And, if needed, invest in a pair of orthotic inserts to further prevent excessive pronation or supination.
Prevention
Pronation forces us to bear most of our weight on the inner border of our feet. Custom-made orthotics gently redistributes the weight so that the entire foot bears its normal share of weight with each step we take. The foot will not twist out at the ankle, but will strike the ground normally when the orthotics is used. This action of the custom-made orthotics will help to prevent shin splints, ankle sprains, knee and hip pain, lower back pain, nerve entrapments, tendonitis, muscle aches, bunions, generalized fatigue, hammer toes, and calluses.
Severs Disease Facts And Figures
Overview
Sever?s disease, also known as calcaneal apophysitis, is a common heel problem affecting children. This heel bone disorder is often painful, though it?s usually temporary and causes no long-term health effects. With Sever?s disease, the Achilles tendon repeatedly pulls on the heel?s growth plate, causing microtrauma (i.e. microfractures), inflammation, and swelling in the affected area. Sever?s disease is similar to Osgood-Schlatter disease, which affects the knee. Inappropriate footwear may be a contributing factor in the onset of this condition.
Causes
This condition is more common in boys than girls. It generally presents between the ages of 9-14 and peaks between ages 10-12 years. This injury can reoccur up until the age of 17, when the growth plate of the calcaneous generally closes. These types of injuries will commonly occur during periods of rapid growth. Sever?s Disease occurs more frequently in child with flat feet, but all children with flat feet will not get Sever?s.
Symptoms
In Sever?s disease, heel pain can be in one or both heels. It usually starts after a child begins a new sports season or a new sport. Your child may walk with a limp. The pain may increase when he or she stands on tiptoe. Your child?s heel may hurt if you squeeze both sides toward the very back. This is called the squeeze test. Your provider may also find that your child?s heel tendons have become tight.
Diagnosis
Low-grade inflammation of the calcaneal apophysis cannot be seen on x-ray. Therefore, although x-rays are often done to rule out bony injuries in children with Sever's disease these x-rays are usually normal. Advanced Sever's disease can be seen on x-ray but usually the problem is treated before it reaches this point. Other diagnostic tests, such as bone scans or MRI's, are not usually required in typical cases of Sever's disease. These, or other tests, may be required to rule out other conditions, such as stress fractures of the calcaneus or other bony abnormalities that can mimic Severs disease.
Non Surgical Treatment
Cold packs: Apply ice or cold packs to the back of the heels for around 15 minutes after any physical activity, including walking.
Shoe inserts: Small heel inserts worn inside the shoes can take some of the traction pressure off the Achilles tendons. This will only be required in the short term.
Medication: Pain-relieving medication may help in extreme cases, but should always be combined with other treatment and following consultation with your doctor).
Anti-inflammatory creams: Also an effective management tool.
Splinting or casting: In severe cases, it may be necessary to immobilise the lower leg using a splint or cast, but this is rare.
Time: Generally the pain will ease in one to two weeks, although there may be flare-ups from time to time.
Correction of any biomechanical issues: A physiotherapist can identify and discuss any biomechanical issues that may cause or worsen the condition.
Education: Education on how to self-manage the symptoms and flare-ups of Sever?s disease is an essential part of the treatment.
Recovery
This condition is self limiting, it will go away when the two parts of bony growth join together, this is natural. Unfortunately, Sever's disease can be very painful and limit sport activity of the child while waiting for it to go away, so treatment is often advised to help relieve it. In a few cases of Sever's disease, the treatment is not successful and these children will be restricted in their activity levels until the two growth areas join, usually around the age of 16 years. There are no known long term complications associated with Sever's disease.
Sever?s disease, also known as calcaneal apophysitis, is a common heel problem affecting children. This heel bone disorder is often painful, though it?s usually temporary and causes no long-term health effects. With Sever?s disease, the Achilles tendon repeatedly pulls on the heel?s growth plate, causing microtrauma (i.e. microfractures), inflammation, and swelling in the affected area. Sever?s disease is similar to Osgood-Schlatter disease, which affects the knee. Inappropriate footwear may be a contributing factor in the onset of this condition.
Causes
This condition is more common in boys than girls. It generally presents between the ages of 9-14 and peaks between ages 10-12 years. This injury can reoccur up until the age of 17, when the growth plate of the calcaneous generally closes. These types of injuries will commonly occur during periods of rapid growth. Sever?s Disease occurs more frequently in child with flat feet, but all children with flat feet will not get Sever?s.
Symptoms
In Sever?s disease, heel pain can be in one or both heels. It usually starts after a child begins a new sports season or a new sport. Your child may walk with a limp. The pain may increase when he or she stands on tiptoe. Your child?s heel may hurt if you squeeze both sides toward the very back. This is called the squeeze test. Your provider may also find that your child?s heel tendons have become tight.
Diagnosis
Low-grade inflammation of the calcaneal apophysis cannot be seen on x-ray. Therefore, although x-rays are often done to rule out bony injuries in children with Sever's disease these x-rays are usually normal. Advanced Sever's disease can be seen on x-ray but usually the problem is treated before it reaches this point. Other diagnostic tests, such as bone scans or MRI's, are not usually required in typical cases of Sever's disease. These, or other tests, may be required to rule out other conditions, such as stress fractures of the calcaneus or other bony abnormalities that can mimic Severs disease.
Non Surgical Treatment
Cold packs: Apply ice or cold packs to the back of the heels for around 15 minutes after any physical activity, including walking.
Shoe inserts: Small heel inserts worn inside the shoes can take some of the traction pressure off the Achilles tendons. This will only be required in the short term.
Medication: Pain-relieving medication may help in extreme cases, but should always be combined with other treatment and following consultation with your doctor).
Anti-inflammatory creams: Also an effective management tool.
Splinting or casting: In severe cases, it may be necessary to immobilise the lower leg using a splint or cast, but this is rare.
Time: Generally the pain will ease in one to two weeks, although there may be flare-ups from time to time.
Correction of any biomechanical issues: A physiotherapist can identify and discuss any biomechanical issues that may cause or worsen the condition.
Education: Education on how to self-manage the symptoms and flare-ups of Sever?s disease is an essential part of the treatment.
Recovery
This condition is self limiting, it will go away when the two parts of bony growth join together, this is natural. Unfortunately, Sever's disease can be very painful and limit sport activity of the child while waiting for it to go away, so treatment is often advised to help relieve it. In a few cases of Sever's disease, the treatment is not successful and these children will be restricted in their activity levels until the two growth areas join, usually around the age of 16 years. There are no known long term complications associated with Sever's disease.
Pain In The Arch Reasons Symptoms And Treatment
Overview
Flat feet are characterized by no arch in the inner foot. It can be a genetic condition or the result of improper body mechanics. Often the whole of the foot will contact the ground. A healthy foot structure supports the body's weight from the bone structure arch; a flat foot is unable to properly support this weight, causing pressure in the ankle, knee and hip joints.
Causes
There are many causes for a high arch (cavus) foot. In the United States, the most common cause for a high arch foot is a form of muscular dystrophy called hereditary sensorimotor neuropathy. Most people recognize this by the more commonly used name of Charcot Marie Tooth disease (CMT). This is a disease of the muscles and the nerves of the legs, and occasionally of the hands, in which certain muscles weaken while others retain their strength. The condition is transmitted as an autosomal dominant condition. This means that 50% of the offspring will statistically inherit the disorder. This is, however, just a statistic. In some families, all the children develop the condition while in others, none inherit it.
Symptoms
If you've ever seen your footprints in the sand and they looked more like bricks than feet, then you probably have flat feet. Simply stated, a flat foot is a foot that does not have an arch when standing. In the medical world, flat feet are associated with "pronated" feet. Pronated is merely the term used to describe the position of the foot when it is flexed upward (dorsiflexed), turned away from the body (abducted), and the heel is rolled outward (everted), all at the same time. A certain amount of pronation is required for normal walking, but too much pronation is often considered a foot's "worst enemy." Over time, excessive pronation can lead to many unpleasant problems including heel pain, bunions, hammertoes, shin splints, and even knee, hip, or back pain. In fact, one orthopedic surgeon discovered that 95% of his total knee replacement patients and 90% of his total hip replacement patients had flat feet. An easy way to tell if you pronate too much is to take a look at your athletic shoes-excessive wearing of the inside heel (arch side of the shoe) as compared to the outside is a classic indication of excessive pronation.
Diagnosis
Flat feet are easy to identify while standing or walking. When someone with flat feet stands, their inner foot or arch flattens and their foot may roll over to the inner side. This is known as overpronation. To see whether your foot overpronates, stand on tiptoes or push your big toe back as far as possible. If the arch of your foot doesn't appear, your foot is likely to overpronate when you walk or run. It can be difficult to tell whether a child has flat feet because their arches may not fully develop until they're 10 years of age.
Non Surgical Treatment
Anti-inflammatory medications such as ibuprofen and aspirin can provide short-term relief from foot pain associated with fallen arches, notes the American Academy of Orthopaedic Surgeons. Doctors sometimes inject the foot with a corticosteroid medication, which acts as an anti-inflammatory, to relieve acute pain. Although medications can provide symptom relief, they do not correct the underlying foot abnormality.

Surgical Treatment
Surgical advances have dramatically improved the ability to alleviate the pain and decreased function that millions of Americans experience due to flat feet. Nevertheless, many patients and even some physicians remain unaware of the new procedures, which are best performed by a foot and ankle specialist who has the applicable training and experience.
Prevention
Warm up properly. This means not only stretching prior to a given athletic event, but a gradual rather than sudden increase in volume and intensity over the course of the training season. A frequent cause of plantar fasciitis is a sudden increase of activity without suitable preparation. Avoid activities that cause pain. Running on steep terrain, excessively hard or soft ground, etc can cause unnatural biomechanical strain to the foot, resulting in pain. This is generally a sign of stress leading to injury and should be curtailed or discontinued. Shoes, arch support. Athletic demands placed on the feet, particularly during running events, are extreme. Injury results when supportive structures in the foot have been taxed beyond their recovery capacity. Full support of the feet in well-fitting footwear reduces the likelihood of injury. Rest and rehabilitation. Probably the most important curative therapy for cases of plantar fasciitis is thorough rest. The injured athlete must be prepared to wait out the necessary healing phase, avoiding temptation to return prematurely to athletic activity.
Stretching Exercises
Calf Stretching in Bed. As you may already know, the first few steps out of bed in the morning can be the worst of the day. Those first few steps can be enough to reaggravate your condition putting you into a cycle of inflammation and pain. The best way to help break that cycle is to stretch your calf before taking those first steps in the morning. When the muscles in your calf are tight, they pull on the heel bone, making your plantar fascia very taut and prone to injury. To help loosen those muscles, take a towel or belt and loop it around the ball of your foot. Keeping your leg straight, gently pull towards your body until you feel a stretch in the lower part of your leg. Hold that for 30 seconds and repeat up to 5 times before taking your first step out of bed. Plantar Fascia Stretching. Loosening up the tissues that are irritated probably makes sense to you, but you may not know how to do so. Luckily, there?s a very simple way. All you have to do is pull your toes up with your hand until you feel a stretch along the ball of your foot. You may feel the stretch anywhere from the ball of your foot to your heel. Holding this position for 30 seconds a few times can make a world of difference in your pain levels. Calf Stretching. I know, it probably seems like overkill, but stretching out the muscles in the lower leg is an integral step to recovery. There are two main muscles in the lower leg that attach to the heel, so we?ll work on stretching them both out. Stand against a wall and slide one leg back, pushing the heel down towards the floor (first picture). When you feel a stretch in the lower part of your leg, hold it for 30 seconds. After those 30 seconds are up, bend your knees until a deeper stretch is felt a bit lower in the leg (second photo). Again, hold this stretch for 30 seconds and repeat this until you?ve done it 3 times on each leg. Who doesn?t love a good massage? I suppose you could pay for someone to rub out the tissues in the bottom of your foot, but if you?re looking for a cheaper alternative, look no further than the humble tennis ball. Placing a tennis ball on the ground and gently rolling it under foot for a few minutes can help loosen up your plantar fascia, making it much less likely to become irritated. Put enough pressure on the ball to get a deep massage. You may feel some soreness, but back off if you feel any pain.Tennis Ball Massage While using the tennis ball is great for keeping things loose, sometimes it?s worth doing some icing at the same time for some inflammation control. Freezing a water bottle and rolling it under your foot for 10 minutes at the end of the day can be a very effective way to keep inflammation in check while staying loose. It might not be the most comfortable thing in the world, but ?Brrr? is better than ?Ouch? any day. One thing to keep in mind is that while these tips have been proven to work, they?re not an instant fix. It can take a few weeks of consistency with them before your pain levels begin to change. If you?re not seeing any improvement after making an honest effort, it may be time to look into some different treatment methods with your doctor such as formal PT, orthotics, a weight-loss plan, or others.
Flat feet are characterized by no arch in the inner foot. It can be a genetic condition or the result of improper body mechanics. Often the whole of the foot will contact the ground. A healthy foot structure supports the body's weight from the bone structure arch; a flat foot is unable to properly support this weight, causing pressure in the ankle, knee and hip joints.
Causes
There are many causes for a high arch (cavus) foot. In the United States, the most common cause for a high arch foot is a form of muscular dystrophy called hereditary sensorimotor neuropathy. Most people recognize this by the more commonly used name of Charcot Marie Tooth disease (CMT). This is a disease of the muscles and the nerves of the legs, and occasionally of the hands, in which certain muscles weaken while others retain their strength. The condition is transmitted as an autosomal dominant condition. This means that 50% of the offspring will statistically inherit the disorder. This is, however, just a statistic. In some families, all the children develop the condition while in others, none inherit it.
Symptoms
If you've ever seen your footprints in the sand and they looked more like bricks than feet, then you probably have flat feet. Simply stated, a flat foot is a foot that does not have an arch when standing. In the medical world, flat feet are associated with "pronated" feet. Pronated is merely the term used to describe the position of the foot when it is flexed upward (dorsiflexed), turned away from the body (abducted), and the heel is rolled outward (everted), all at the same time. A certain amount of pronation is required for normal walking, but too much pronation is often considered a foot's "worst enemy." Over time, excessive pronation can lead to many unpleasant problems including heel pain, bunions, hammertoes, shin splints, and even knee, hip, or back pain. In fact, one orthopedic surgeon discovered that 95% of his total knee replacement patients and 90% of his total hip replacement patients had flat feet. An easy way to tell if you pronate too much is to take a look at your athletic shoes-excessive wearing of the inside heel (arch side of the shoe) as compared to the outside is a classic indication of excessive pronation.
Diagnosis
Flat feet are easy to identify while standing or walking. When someone with flat feet stands, their inner foot or arch flattens and their foot may roll over to the inner side. This is known as overpronation. To see whether your foot overpronates, stand on tiptoes or push your big toe back as far as possible. If the arch of your foot doesn't appear, your foot is likely to overpronate when you walk or run. It can be difficult to tell whether a child has flat feet because their arches may not fully develop until they're 10 years of age.
Non Surgical Treatment
Anti-inflammatory medications such as ibuprofen and aspirin can provide short-term relief from foot pain associated with fallen arches, notes the American Academy of Orthopaedic Surgeons. Doctors sometimes inject the foot with a corticosteroid medication, which acts as an anti-inflammatory, to relieve acute pain. Although medications can provide symptom relief, they do not correct the underlying foot abnormality.
Surgical Treatment
Surgical advances have dramatically improved the ability to alleviate the pain and decreased function that millions of Americans experience due to flat feet. Nevertheless, many patients and even some physicians remain unaware of the new procedures, which are best performed by a foot and ankle specialist who has the applicable training and experience.
Prevention
Warm up properly. This means not only stretching prior to a given athletic event, but a gradual rather than sudden increase in volume and intensity over the course of the training season. A frequent cause of plantar fasciitis is a sudden increase of activity without suitable preparation. Avoid activities that cause pain. Running on steep terrain, excessively hard or soft ground, etc can cause unnatural biomechanical strain to the foot, resulting in pain. This is generally a sign of stress leading to injury and should be curtailed or discontinued. Shoes, arch support. Athletic demands placed on the feet, particularly during running events, are extreme. Injury results when supportive structures in the foot have been taxed beyond their recovery capacity. Full support of the feet in well-fitting footwear reduces the likelihood of injury. Rest and rehabilitation. Probably the most important curative therapy for cases of plantar fasciitis is thorough rest. The injured athlete must be prepared to wait out the necessary healing phase, avoiding temptation to return prematurely to athletic activity.
Stretching Exercises
Calf Stretching in Bed. As you may already know, the first few steps out of bed in the morning can be the worst of the day. Those first few steps can be enough to reaggravate your condition putting you into a cycle of inflammation and pain. The best way to help break that cycle is to stretch your calf before taking those first steps in the morning. When the muscles in your calf are tight, they pull on the heel bone, making your plantar fascia very taut and prone to injury. To help loosen those muscles, take a towel or belt and loop it around the ball of your foot. Keeping your leg straight, gently pull towards your body until you feel a stretch in the lower part of your leg. Hold that for 30 seconds and repeat up to 5 times before taking your first step out of bed. Plantar Fascia Stretching. Loosening up the tissues that are irritated probably makes sense to you, but you may not know how to do so. Luckily, there?s a very simple way. All you have to do is pull your toes up with your hand until you feel a stretch along the ball of your foot. You may feel the stretch anywhere from the ball of your foot to your heel. Holding this position for 30 seconds a few times can make a world of difference in your pain levels. Calf Stretching. I know, it probably seems like overkill, but stretching out the muscles in the lower leg is an integral step to recovery. There are two main muscles in the lower leg that attach to the heel, so we?ll work on stretching them both out. Stand against a wall and slide one leg back, pushing the heel down towards the floor (first picture). When you feel a stretch in the lower part of your leg, hold it for 30 seconds. After those 30 seconds are up, bend your knees until a deeper stretch is felt a bit lower in the leg (second photo). Again, hold this stretch for 30 seconds and repeat this until you?ve done it 3 times on each leg. Who doesn?t love a good massage? I suppose you could pay for someone to rub out the tissues in the bottom of your foot, but if you?re looking for a cheaper alternative, look no further than the humble tennis ball. Placing a tennis ball on the ground and gently rolling it under foot for a few minutes can help loosen up your plantar fascia, making it much less likely to become irritated. Put enough pressure on the ball to get a deep massage. You may feel some soreness, but back off if you feel any pain.Tennis Ball Massage While using the tennis ball is great for keeping things loose, sometimes it?s worth doing some icing at the same time for some inflammation control. Freezing a water bottle and rolling it under your foot for 10 minutes at the end of the day can be a very effective way to keep inflammation in check while staying loose. It might not be the most comfortable thing in the world, but ?Brrr? is better than ?Ouch? any day. One thing to keep in mind is that while these tips have been proven to work, they?re not an instant fix. It can take a few weeks of consistency with them before your pain levels begin to change. If you?re not seeing any improvement after making an honest effort, it may be time to look into some different treatment methods with your doctor such as formal PT, orthotics, a weight-loss plan, or others.
Posterior Tibial Tendon Dysfunction (PTTD) Treatments And Causes
Overview
Adult acquired flatfoot deformity (AAFD), embraces a wide spectrum of deformities. AAFD is a complex pathology consisting both of posterior tibial tendon insufficiency and failure of the capsular and ligamentous structures of the foot. Each patient presents with characteristic deformities across the involved joints, requiring individualized treatment. Early stages may respond well to aggressive conservative management, yet more severe AAFD necessitates prompt surgical therapy to halt the progression of the disease to stages requiring more complex procedures. We present the most current diagnostic and therapeutic approaches to AAFD, based on the most pertinent literature and our own experience and investigations. 
Causes
There are multiple factors contributing to the development of this problem. Damage to the nerves, ligaments, and/or tendons of the foot can cause subluxation (partial dislocation) of the subtalar or talonavicular joints. Bone fracture is a possible cause. The resulting joint deformity from any of these problems can lead to adult-acquired flatfoot deformity. Dysfunction of the posterior tibial tendon has always been linked with adult-acquired flatfoot deformity (AAFD). The loss of active and passive pull of the tendon alters the normal biomechanics of the foot and ankle. The reasons for this can be many and varied as well. Diabetes, high blood pressure, and prolonged use of steroids are some of the more common causes of adult-acquired flatfoot deformity (AAFD) brought on by impairment of the posterior tibialis tendon. Overstretching or rupture of the tendon results in tendon and muscle imbalance in the foot leading to adult-acquired flatfoot deformity (AAFD). Rheumatoid arthritis is one of the more common causes. About half of all adults with this type of arthritis will develop adult flatfoot deformity over time. In such cases, the condition is gradual and progressive. Obesity has been linked with this condition. Loss of blood supply for any reason in the area of the posterior tibialis tendon is another factor. Other possible causes include bone fracture or dislocation, a torn or stretched tendon, or a neurologic condition causing weakness.
Symptoms
Posterior tibial tendon insufficiency is divided into stages by most foot and ankle specialists. In stage I, there is pain along the posterior tibial tendon without deformity or collapse of the arch. The patient has the somewhat flat or normal-appearing foot they have always had. In stage II, deformity from the condition has started to occur, resulting in some collapse of the arch, which may or may not be noticeable. The patient may feel it as a weakness in the arch. Many patients initially present in stage II, as the ligament failure can occur at the same time as the tendon failure and therefore deformity can already be occurring as the tendon is becoming symptomatic. In stage III, the deformity has progressed to the extent where the foot becomes fixed (rigid) in its deformed position. Finally, in stage IV, deformity occurs at the ankle in addition to the deformity in the foot.
Diagnosis
The history and physical examination are probably the most important tools the physician uses to diagnose this problem. The wear pattern on your shoes can offer some helpful clues. Muscle testing helps identify any areas of weakness or muscle impairment. This should be done in both the weight bearing and nonweight bearing positions. A very effective test is the single heel raise. You will be asked to stand on one foot and rise up on your toes. You should be able to lift your heel off the ground easily while keeping the calcaneus (heel bone) in the middle with slight inversion (turned inward). X-rays are often used to study the position, shape, and alignment of the bones in the feet and ankles. Magnetic resonance (MR) imaging is the imaging modality of choice for evaluating the posterior tibial tendon and spring ligament complex.
Non surgical Treatment
Because of the progressive nature of PTTD, early treatment is advised. If treated early enough, your symptoms may resolve without the need for surgery and progression of your condition can be arrested. In contrast, untreated PTTD could leave you with an extremely flat foot, painful arthritis in the foot and ankle, and increasing limitations on walking, running, or other activities. In many cases of PTTD, treatment can begin with non-surgical approaches that may include. Orthotic devices or bracing. To give your arch the support it needs, your foot and ankle surgeon may provide you with an ankle brace or a custom orthotic device that fits into the shoe. Immobilization. Sometimes a short-leg cast or boot is worn to immobilize the foot and allow the tendon to heal, or you may need to completely avoid all weight-bearing for a while. Physical therapy. Ultrasound therapy and exercises may help rehabilitate the tendon and muscle following immobilization. Medications. Nonsteroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen, help reduce the pain and inflammation. Shoe modifications. Your foot and ankle surgeon may advise changes to make with your shoes and may provide special inserts designed to improve arch support. 
Surgical Treatment
If surgery is necessary, a number of different procedures may be considered. The specifics of the planned surgery depend upon the stage of the disorder and the patient?s specific goals. Procedures may include ligament and muscle lengthening, removal of the inflamed tendon lining, tendon transfers, cutting and realigning bones, placement of implants to realign the foot and joint fusions. In general, early stage disease may be treated with tendon and ligament (soft-tissue) procedures with the addition of osteotomies to realign the foot. Later stage disease with either a rigidly fixed deformity or with arthritis is often treated with fusion procedures. If you are considering surgery, your doctor will speak with about the specifics of the planned procedure.